Health benefits of New Urbanism




Urban design factors can affect public health in several ways, including physical activity, traffic accident risk, pollution exposure, access to health resources, mental health and affordability, which affects households’ ability to afford other critical goods, such as healthy food and medical care.
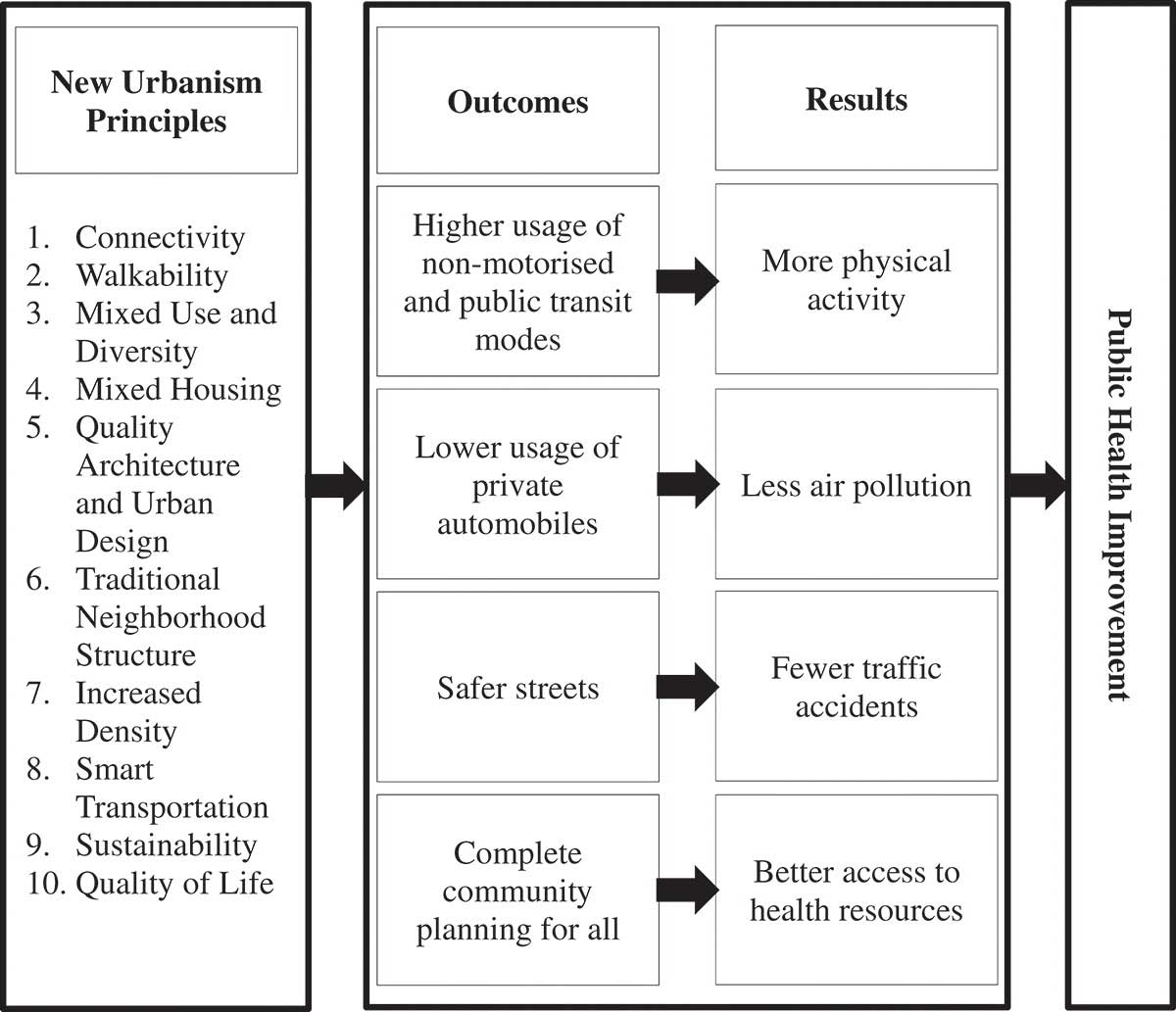
The aim of this study was to evaluate the potential impacts on the public health of several urban design features categorized under 10 New Urbanism principles of walkable blocks and streets; connectivity; mixed use and diversity; mixed housing; quality architecture and urban design; traditional neighborhood structure; increased density; smart transportation; sustainability; and quality of life.
Public health data for counties across the United States was obtained from the County Health Rankings and Roadmaps (CHR&R) program, a collaboration of the Robert Wood Johnson Foundation and the University of Wisconsin Population Health Initiative.
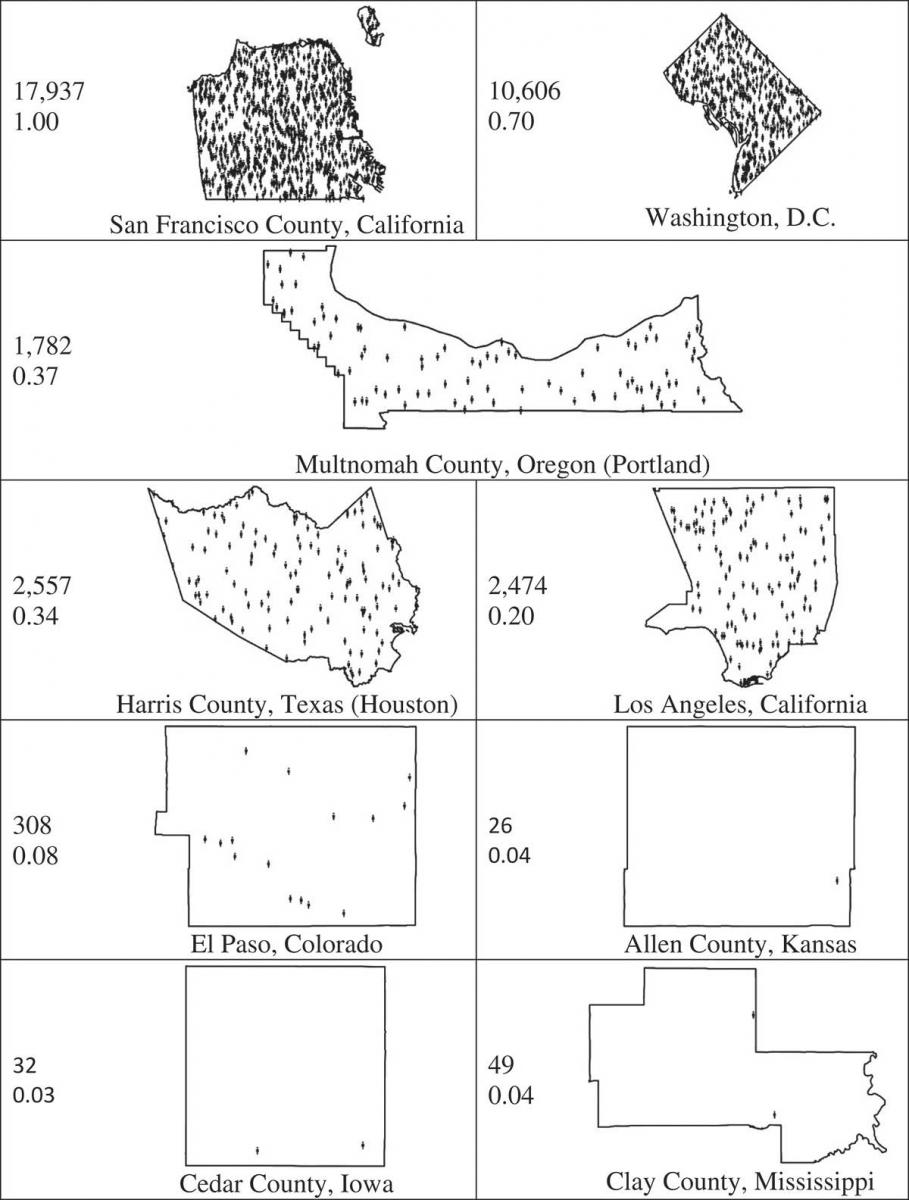
Los Angeles County, California (Los Angeles); Harris County, Texas (Houston); and El Paso County, Colorado, were included as large urban centers. Clay County, Mississippi, and Allen County, Kansas, were included as mixed locations for socio-economic factors. Cedar County, Iowa, was included as a typical rural county. The final three regions—San Francisco County, California (San Francisco); Washington, DC; and Multnomah County, Oregon (Portland)—contain cities ranked among the smartest cities in North America, based on a key set of assessment factors linked to sustainability, technology-enabled innovation and citizen participation.
Principles 1 and 2: Walkability and connectivity
The results of the analysis clearly indicate a very strong relationship between (a) walkability and health and (b) connectivity and health, the first two principles mentioned above. In addition, the counties that have a higher value of walkability and connectivity (San Francisco, Portland and Washington, DC) consistently rank higher across the health and wellness measures. This indicates that urban forms manifesting gridded networks and smaller blocks, allowing for more intersections and enabling pedestrians to walk a variety of routes from their points of origin and destinations, have a promotive effect on health and wellness and embody a key design characteristic of smart cities. Study counties reporting a higher incidence of obesity and greater prevalence of type 2 diabetes have much lower connectivity indicator (CI) values, requiring automobiles for transportation.
A dense grid network—whether the grid is regular or irregular—with smaller block size and intersection spacing, provides multiple choices and more freedom for pedestrians to walk any origin-destination pairs. Pedestrians have choices of different routes and can discover more at each junction, while their routes will be shorter because they can avoid out-of-direction traffic. Smaller blocks provide more places where automobiles can stop to allow pedestrians to cross streets. Furthermore, smaller blocks that have reduced distances between two consecutive intersections will distribute car traffic among the roads more evenly as opposed to funneling all car traffic onto a few major roads, which is typical of a low-CI city design. Studies have shown that small block size and a dense grid roadway network offer a different experience, encourage the use of other means of transportation, and promote health and wellness. Smaller blocks reduce distances between origin-destination pairs, a key shortcoming of conventional expressway design.
Primary constraints on the data analysis and evaluation are the probable roles of socio-economic and demographic variables. Furthermore, there are relatively few walkable cities in the US, which limited the sample size for this study. Hence, the data analysis approach should be used as a guide for the purpose of comparative analysis, not for developing a comprehensive mathematical model. However, this study also referred to Allan Jacobs’s data analysis of city street design as a secondary resource, which is supported by data and drawings representing more than 40 world cities, revealing that higher intersection density promotes a higher level of walking, which aligns with this study’s conclusion.
Literature reviews were conducted to assess the health impacts of the other eight principles.
Principle 3: Mixed use and diversity
Mixed-use developments bring origin-destination pairs closer, enhancing urban vibrancy, increasing physical activity and promoting the use of active transportation, resulting in improved health outcomes and reduced travel distance, minimizing the need for private automobiles. Frank, Andresen, and Schmid (2004) revealed an association between land use and physical fitness in a study involving the 13 counties of the metropolitan Atlanta region, and concluded that the likelihood of being obese reduces as the mix of land use increases. The study estimated that each additional hour spent in an automobile per day was associated with a 6 percent increase in the likelihood of obesity. Conversely, each additional kilometre walked per day was associated with a 4.8 percent reduction in the likelihood of obesity.
The health benefits accrued with mixed-use developments are attributable to people walking and riding bicycles more than in typical suburban environments with segregated land use. Saelens, Sallis, and Frank (2003) presented evidence indicating that residents in communities that have higher-density developments, greater connectivity and more mixed-use land walk and/or cycle more for utilitarian purposes as opposed to low-density developments with lower levels of connectivity and with widely separated single land uses.
Principle 4: Mixed housing
Mixed housing aims to meet the basic needs of all residents to live, work and play, regardless of income level, age, socio-economic standing or culture. Complete communities is an urban-planning concept that respects the needs of all residents— regardless of their income, culture, age or ideas. Considering that the focus of the health quality of residents is more on prevention, a range of housing choices that enables older adults to age in place is vital. Affordable housing, safe outdoor spaces, places that encourage active living with inexpensive and convenient transportation options, opportunities for social participation and community leadership, and accessible health and wellness services are among the important criteria to promote for developing age-friendly communities. Residential areas in communities should include affordable housing for low-income populations and the elderly, so they can spend more income on their health and well-being. As stated by the co-founder of the CNU, Peter Calthorpe (1999),
We should no longer isolate the poor in the inner city and segregate the middle class in the suburbs. It implies limiting additional public housing in low-income neighborhoods, and instead scattering public housing throughout the region and fostering inclusionary zoning in the suburbs.
Principle 5: Quality architecture and urban design
Indoor environments, as designed and operated, are linked to adverse effects on public health (Guenther and Vittori, 2008). As it relates to outdoor environments, the transportation network is the framework upon which cities are built and shapes the growth and evolution of cities. Conventional road design relies on wide roads and highways segmenting cities into parts and promotes automobile traffic while offering no support for non-motorized transportation. This results in traffic congestion and pollution and minimizes walking, thereby resulting in negative impacts on public health. An interactive public realm offers opportunities for people to meet, move, relax and observe through a network of well-connected, narrower streets and appropriately arranged streetscapes that encompass a series of open spaces and nodes of activity. The health-promotive urban design should not lay out streets only as conduits to move traffic but rather as enablers for residents to walk, socialize and play. Wide roads, by design, break connectivity within the city. It is known that roads have diseconomy of scale as opposed to other services (Kulash, Anglin, and Marks, 1990).In other words, four two-lane roads function better than one eight-lane road for pedestrians and automobiles, because there will be more choices for turning and because traffic distributes more evenly on multiple streets rather than being funneled onto a few wide roads, making it easier for pedestrians to walk, navigate and cross streets.
Principle 6: Traditional neighborhood structure
New Urbanism should not be framed merely as a conservative approach to recapture outdated traditions while ignoring the issues of our time. However, replacing cul-de-sacs and auto-oriented shopping malls with traditional urban design, along with instituting diversity and the principles of regionalism, will take cities back from cars and return them to people (Calthorpe et al.,1999). Traditional urban design, while considering the needs of modern life, attempts to resurrect the sense of place and community in neighborhoods with its attendant mental- and physical-health-quality improvements.
The Michigan Land Use Institute (2006) describes the traditional neighborhood structure principle of New Urbanism as neighborhoods with definite centers and edges, including public spaces near the center. Each neighborhood contains a range of uses and densities within a 10-minute walk. Traditional neighborhood design promotes compact housing, a grid street network with short blocks and mixed use. Zuniga-Teran et al. (2017) performed a comparative analysis of four different neighborhood designs in Tucson, Arizona—(a) traditional development; (b) suburban development; (c) cluster housing development; and (d) enclosed community—and evaluated the level of walkability and its effects on physical activity and well-being. The study concluded that traditional development strongly correlated with the highest value for walkability, whether for recreation or transportation. Suburban development indicated significant association and the highest mean values for mental health and well-being. Cluster housing was ranked the highest for social interactions with neighbors and for perceived safety from crime. Enclosed community did not obtain the highest mean value for any well-being benefit in any of these categories.
Principle 7: Increased density
High-density developments within the context of a compact city that promote vertical growth and mixed use and that create limits to urban expansion bring origins closer to destinations and therefore make places more walkable, leading to many economic, social, environmental and health benefits. In contrast, urban sprawl tends to create resident dependency on private automobiles, an increase in vehicle miles travelled (VMT). Adverse impacts on health result from the air pollution associated with more automobile traffic in an urban sprawl environment.
Evidence exists that residents in more compact areas have more active travel and therefore lower body mass indexes (BMIs) and lower probabilities of obesity and chronic diseases (Ewing and Cervero, 2010).In a study, Ewing et al. (2014) concluded that urban and suburban areas with more compact areas are linked with ameliorative effects on obesity and chronic diseases. The study indicated that sprawl is associated with obesity, high blood pressure or other health conditions, but did not elaborate on the type of sprawl associated with adverse health effects, recommending additional epidemiologic research using longitudinal cohorts for the study.
In a study prepared by Giles-Corti et al (2014) for the National Heart Foundation of Australia, the potential impact of low-density developments on physical activity and health was investigated. Extensive literature review and meta data analysis concluded that those who lived in lower-density neighborhoods, or who were perceived as living in lower-density areas, walked less than those in the higher-density areas. The same study also revealed associative evidence between living in lower-density areas and increased overweight and obese adults and adolescents, although such a relationship with younger children was inconclusive. Moreover, the study revealed a greater positive association between behavioral changes geared towards walking and cycling among individuals living in higher densities compared to those living in low-density developments that are more dependent on automobiles for transportation. It is noteworthy to mention that activity cenrters in Portland, Oregon, are highly walkable. The reason that Portland’s walkability score is not as high as expected, is because the analysis considered the entirety of Multnomah County, where Portland is located, and the low-density character of the county’s suburbs brought its overall average walkability score to a lower value.
Principle 8: Smart transportation
City planners and public-health experts are beginning to evaluate the potential of smart technologies to directly address health- and wellness-related benefits as part of a foundational architecture concept for smart cities. However, it is important to note that technology is merely an enabler and effective only when applied with best-practice transportation planning and urban design. Smart transportation is about moving people as opposed to cars. Smart city design considerations should address health- and wellness-related priorities and require establishing health-related public policies at the local levels by the city administrators to create healthy environments and surroundings and to establish service offerings aimed at promoting citizen empowerment and participation at the community level (Andrade et al. (2017).
Multimodal transportation system
A recent study by Frederick, Riggs, and Gilderbloom (2017) examined 148 US counties and their metropolitan statistical areas by measuring 12 public-health and quality-of-life indicators against commute mode diversity (CMD). It found a positive relationship between metropolitan areas that have fewer workers commuting by SOV with (a) better health conditions and healthier behaviors evaluated on the Gallup/Healthway’s Well-Being Index; (b) more leisure quality reported by Sperling’s Cities Ranked and Rated; (c) more access to exercise reported by the Environmental Systems Research Institute; (d) less sedentary living and obesity reported in the CDC Diabetes Interactive Atlas; and (e) more years of potential life lost (an indicator of longevity and overall health) and higher birth weights (an indicator of infant health), as reported by the National Center for Health Statistics. The finding revealed powerful statistical evidence of cities offering multimodal travel environments having a positive impact on public health as well as many other sociological, geographical and economic concerns, including race, density, latitude, education and income. The main components of a multimodal system are walking, cycling and public transportation. Researchers have evaluated the positive impact of public transportation on health and wellness and assessed ways to incorporate these public health-related considerations as part of formulating transportation policy (Litman, 2016). These and other similar studies have evaluated the significant behavioral changes, such as walking, cycling, the use of public transit and lower ownership of automobiles, associated with a qualitative improvement in health and wellness (Bailey, Mokhtarian, and Little, 2008); (Ohland and Poticha, 2009).
Need for traffic and roadway standards to encourage multimodal transportation
One of the problems associated with implementing best-practice urban design relates to the tools being applied in conventional traffic engineering to evaluate development and traffic conditions. An important aspect of this research is the tools applied to measure connectivity and walkability to evaluate the transportation systems. Traffic engineers, in many cases, have used other tools, such as link volume-to-capacity (V/C) ratio, intersection level of service or related measurements, to ease mobility for cars. However, the focus remains on increasing the roadway and intersection capacity to solve congestion instead of implementing a well-connected network to accommodate all modes of transportation. Transportation design has segregated people and cars under the guise of safety, with an emphasis on wider and larger roadways, which are fundamentally anti-pedestrian. As a result, wider roads and expressways limit accessibility, and large metropolitan centers become increasingly dependent on automobile transportation (Jacobs, 2005).
Traffic safety
Given the importance of traffic safety and its relationship to public health, this study examined the motor-vehicle crash death rate by each county studied as an additional measure and analyzed its relationship with roadway connectivity and walkability in the correlation analysis. The results indicate another corollary benefit of the interconnected roadway networks and walkable places in the study counties, demonstrating better traffic safety and reporting fewer fatal accidents.
Principles 9 and 10: Sustainability and quality of life
Numerous studies have defined smart cities not only by use of technology but also a focus on sustainability and as the crucibles for promoting health and wellness as part of the broader people-centric design and use of technologies. What determines a smart city should be not only how all the elements in the city, including buildings, automobiles, trees, parking and trash cans, are interconnected by technology, but also how they integrate how places and people are well connected as communities by urban design. Environmentally friendly smart cities aim not only at the proximate goals of energy efficiency and pollution prevention but also at the ultimate goal of sustainable cities and communities, which, according to United Nation Development Program (UNDP), means ‘ensuring access to safe and affordable housing, and upgrading slum settlements. It also involves investment in public transport, creating green public spaces, and improving urban planning and management in a way that is both participatory and inclusive (UNDP, 2018).
Smart health is a requirement of smart and sustainable cities. Researchers have proposed the concept of smart health (s-health) as an extension of electronic health (e-health), which is the context-aware complement of mobile health within smart cities, and they have approached this concept as an opportunity to exploit the power of mobile technologies for the more efficient and effective delivery of health care services (Solanas et al., 2014).
Conclusion
The study undertook a systematic investigation of the role of 10 New Urbanism principles on public health and wellness. The impact of the first two principles of New Urbanism, walkability and connectivity, were evaluated by comparing selected US counties. Health condition scores for the selected health and wellness measures for the study regions that included Washington, DC, San Francisco, California, and Portland, Oregon, were consistently higher than other regions included in the study. These regions also scored high on various connectivity indicators that were measured and scored high for intersection density, which is a key design measure indicative of walkability. Higher intersection density and roadway connectivity with narrower roads result in an urban form that induces behavioral changes that promote the use of non-motorized modes of transportation and a higher level of physical activity, bringing with them the attendant health and wellness benefits.
Literature reviews were also conducted to analyze the impact of the other eight New Urbanism principles on public health. Available evidence indicates that residents in mixed-use areas walk and/or cycle more frequently and have better health. This study showed that higher density areas can bring origin and destination pairs closer, and therefore positively affect Policy measures to revise the auto-centric level-of-service tools applied by conventional roadway and traffic engineering standards to make cities more pedestrian- and transit-friendly, resulting in positive impacts on health and wellness.
Traffic safety goals are better attained when cities are more walkable and have higher levels of roadway connectivity. The principles of New Urbanism improve the design and functionalities of the cities as well as public health and wellness and should be a guide for policy makers and practitioners for smart city-development projects. Further research is warranted to apply the influence of socio-economic and demographic variables, particularly income, and compare them with the physical environment’s effects on public health. Moreover, given that New Urbanism principles result in communities that provide people with the opportunity for more social interaction, effects on mental health, including stress, anxiety and depression, are other important topics of research.
This article is an edited version of a study published in the Journal of Urban Design on January 14, 2019.
References
- Andrade, E. A., M. C. T. Franceschini, D. S. Portes, L. B. C. E. Santos, S. R. A. E. Sousa, and V. L. Luiza. 2017. “The Right to the City and International Urban Agendas: A Document Analysis.” Ciencia & saude coletiva 22 (12): 3849–3858. doi:10.1590/1413-81232017228.29642016.
- Bailey, L., P. Mokhtarian, and A. Little 2008. The Broader Connection between Public Transportation, Energy Conservation and Greenhouse Gas Reduction. ICF International. Requested by: American Public Transportation Association. https://www.apta.com/gap/policyresearch/Documents/land_use.pdf
- Caliper Corporation. 2018. Travel Demand Modeling with TransCAD 8. Newton, MA. Accessed March 3 2018. www.caliper.com.
- Calthorpe P. 1999. “Afterword.” In Charter of the New Urbanism, edited by R. Arendt et al., 177–180. New York and London: McGraw-Hill.
- Cohen, B. 2013. The 10 Smartest Cities in North America. Fast Company. Accessed November 14 2013.
- Congress of New Urbanism. Accessed September 20 2018. https://www.cnu.org/resources/what-new-urbanism.
- County Health Ranking (CHR). 2017. The County Health Ranking and Roadmap Program. Madison, WI: University of Wisconsin Population Health Institute.
- Creatore, M., R. Glazier, R. Moineddin, G. Fazli, A. Johns, P. Gozdyra, F. Matheson, et al. 2016. “Association of Neighborhood Walkability with Change in Overweight, Obesity, and Diabetes.” JAMA : the Journal of the American Medical Association 315 (20): 2211. doi:10.1001/jama.2016.5898.
- Ding, D., K. D. Lawson, T. L. Lolbe-Alexander, E. A. Finkelstein, P. T. Katzmarzyk, and M. Pratt. 2016. “The Economic Burden of Physical Inactivity: A Global Analysis of Major Non-Communicable Diseases.” Lancet 388: 1311–1324. doi:10.1016/S0140-6736(16)30383-X.
- Ewing, R., and R. Cervero. 2010. “Travel and the Built Environment.” Journal of the American Planning Association 76 (3): 265–294. doi:10.1080/01944361003766766.
- Ewing, R., G. Meakins, S. Hamidi, and A. Nelson. 2014. “Relationship between Urban Sprawl and Physical Activity, Obesity, and Morbidity – Update and Refinement.” Health & Place 26: 118–126. doi:10.1016/j.healthplace.2013.12.008.
- Frank, D., A. Andresen, and L. Schmid. 2004. “Obesity Relationships with Community Design, Physical Activity, and Time Spent in Cars.” American Journal of Preventive Medicine 27 (2): 87–96. doi:10.1016/j.amepre.2004.04.011.
- Frederick, C., W. Riggs, and J. Gilderbloom. 2017. “Commute Mode Diversity and Public Health: A Multivariate Analysis of 148 US Cities.” International Journal of Sustainable Transportation V12 (1): 1–11.
- Giles-Corti, B., P. Hooper, S. Foster, M. Koohsari, and J. Francis. 2014. Low Density Development: Impacts on Physical Activity and Associated Health Outcomes. Heart Foundation.
- Giles-Corti, B., A. Vernez-Moudon, R. Reis, G. Turrell, A. Dannenberg, H. Badland, S. Foster, et al. 2016. “Urban Design, Transport, and Health.” The Lancet. doi:10.1016/S0140-6736(16)30066-6.
- Guenther, R., and G. Vittori. 2008. Sustainable Healthcare Architecture. New Jersey: John Wiley and Sons.
- Hamer, M., and E. Stamatakis. 2010. “Objectively Assessed Physical Activity, Fitness and Subjective Wellbeing.” Mental Health Physical Activity 3 (2): 67–71. doi:10.1016/j.mhpa.2010.09.001.
- Jacobs, A. B. 1995. Great Streets. Cambridge, MA: MIT Press.
- Jeste, D., D. Blazer, K. Buckwalter, K. Cassidy, L. Fishman, L. Gwyther, S. Levin, et al. 2016. “Age-Friendly Communities Initiative: Public Health Approach to Promoting Successful Aging.” The American Journal of Geriatric Psychiatry 24 (12): 1158–1170. doi:10.1016/j.jagp.2016.07.021.
- Katapally, T. R., J. Bhawra, S. T. Leatherdale, L. Ferguson, J. Longo, D. Rainham, R. Larouche, and N. Osgood. 2018. “The SMART Study, a Mobile Health and Citizen Science Methodological Platform for Active Living Surveillance, Integrated Knowledge Translation, and Policy Interventions: Longitudinal Study.” JMIR Public Health Surveil 4 (1): e31. doi:10.2196/publichealth.8953.
- Kulash, W., J. Anglin, and D. Marks 1990. Traditional Neighborhood Development: Will the Traffic Work? Development. 21, July/August, 21–24. doi:10.1099/00221287-136-2-327
- Laverly, A. A., E. Webb, E. P. Vamos, and C. Millett. 2018. “Associations of Increase in Public Transport Use with Physical Activity and Adiposity in Older Adults.” International Journal of Behavioral Nutrition and Physical Activity 15 (1): 31. doi:10.1186/s12966-018-0660-x.
- Litman, T. 2016. Evaluating Public Transportation Health Benefits. Victoria Transport Policy Institute. Canada.
- Michigan Land Use Institute. 2006. Accessed September 20 2018
- National Research Council (US); Institute of Medicine (US). Editors: Steven H Woolf and Laudan Aron. 2013. U.S. Health in International Perspective, Shorter Lives, Poorer Health. Washington, DC: National Academies Press (US). ISBN-13: 978-0-309-26414-3, ISBN-10: 0-309-26414-6.
- Ohland, G., and S. Poticha. 2009. Street Smart: Street Cars and Cities in the Twenty-First Century. 2nd. Eds G.Ohland and S. Poticha. Reconnecting America.
- Penedo, F. J., and J. R. Dahn. 2005. “Exercise and Wellbeing: A Review of Mental and Physical Health Benefits Associated with Physical Activity.” Current Opinion in Psychiatry 18 (2): 189–193. doi:10.1097/00001504-200503000-00013.
- Public Health Agency of Canada. 2017. Designing Healthy Living. The Chief Public Health Officer’s Report on the State of Public Health in Canada.
- Saelens, B., J. Sallis, and L. Frank. 2003. “Environmental Correlates of Walking and Cycling: Findings from the Transportation, Urban Design, and Planning Literatures.” Annals of Behavioral Medicine 25: 80–91. Source: PubMed. doi:10.1207/S15324796ABM2502_03·.
- Sallis, J., E. Cerin, T. Conway, M. Adams, L. Frank, M. Pratt, D. Salvo, et al. 2016. “Physical Activity in Relation to Urban Environments in 14 Cities Worldwide: A Cross-Sectional Study.” The Lancet 387: 2207–2217. doi:10.1016/S0140-6736(15)01284-2.
- Solanas, A., C. Patsakis, M. Conti, I. S. Vlachos, V. Ramos, F. Falcone, O. Postolache, et al. 2014. “Smart Health: A Context-Aware Health Paradigm within Smart Cities.” IEEE Communications Magazine 52 (8): 74–81. doi:10.1109/MCOM.2014.6871673.
- Stephens, T. 1988. “Physical Activity and Mental Health in the United States and Canada: Evidence from Four Population Surveys.” Preventive Medicine 17 (1): 35–47. doi:10.1016/0091-7435(88)90070-9.
- United Nation Development Programme. Sustainable Development Goals. Goal 11: Sustainable Cities and Communities. Accessed November 3, 2018.
- World Health Organization (WHO). 2018. Fact Sheet: Physical Activity.
- Zuniga-Teran, A., B. Orr, R. Gimblett, N. Chalfoun, D. Guertin, and S. Marsh. 2017. “Neighborhood Design, Physical Activity, and Wellbeing: Applying the Walkability Model.” International Journal of Environmental Research and Public Health 14 (1), 76